Oral health in adults over 60 is shaped by forces that are entirely distinct from those affecting younger patients — forces that interact with each other and with the rest of the body in ways that require an adapted clinical approach. Yet many older adults are managed with the same protocols as younger patients: a twice-yearly cleaning, a reminder to floss more, and a fluoride toothpaste recommendation.
That approach misses most of what matters in geriatric oral health. Here is what actually changes after 60, and what to do about it.
Changes That Come With Age
Enamel becomes thinner and more brittle. Over a lifetime of chewing, enamel wears down on the biting surfaces. This flattening of the chewing surface is called attrition and is visible on X-rays and clinical examination. Thinner enamel is more susceptible to cracking and fracture — which is why unexplained tooth fractures increase in frequency after 60.
Dentin darkens. As the inner layer of the tooth (dentin) ages, it becomes denser and progressively darker. This is why even well-maintained older teeth tend to have a more yellow or gray tone than younger teeth — not from staining alone, but from intrinsic darkening of the tooth structure.
Gum recession exposes root surfaces. Over decades, gum tissue may recede from the crown of the tooth, exposing the cementum-covered root surface below. Root surfaces are softer than enamel, more susceptible to decay, and more sensitive to temperature and sweet foods.
Salivary flow decreases. This is largely medication-driven rather than an inevitable consequence of aging itself. Older adults take more medications, and more medications means more xerostomia. The oral consequences — accelerated decay, increased infection risk, difficulty swallowing — compound over time.
Existing restorations age out. Fillings placed 20, 30, or 40 years ago were often silver amalgam. These restorations have finite lifespans, and as they age, they expand and contract with temperature changes, creating micro-fractures in surrounding tooth structure. Watching for failing restorations is a priority in older patients’ care.
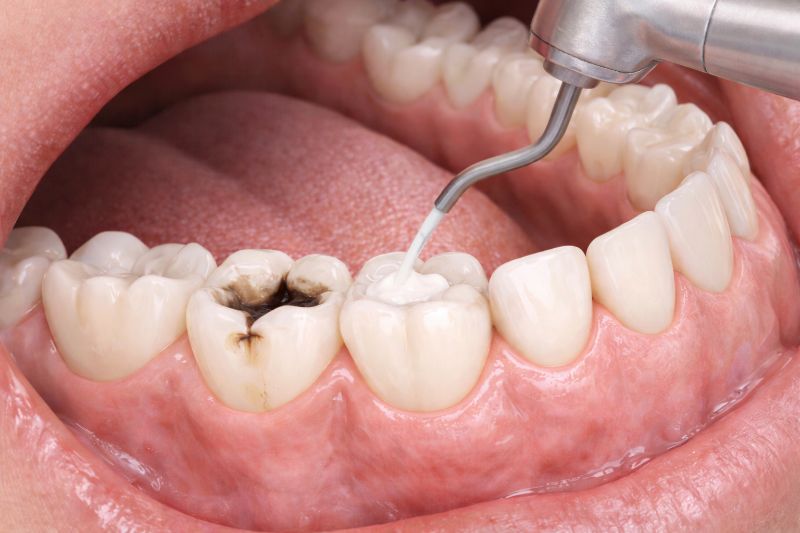
Root Surface Decay: The Defining Dental Threat After 60
Root surface caries — cavities on the exposed root surfaces created by gum recession — is the most prevalent and distinctive dental disease of older adults. Root surfaces are covered by cementum, a calcified tissue that is significantly softer than enamel and requires only a pH of around 6.7 to begin demineralizing (compared to 5.5 for enamel). This means acids that barely threaten enamel actively dissolve root surfaces.
Root caries often develops rapidly — within months in high-risk patients — and in locations that are difficult for patients to see or notice until the decay is advanced. It tends to spread circumferentially around the root rather than downward, making it especially destructive.
Prevention and management:
- Prescription fluoride toothpaste (5,000 ppm) — the single most impactful intervention for root caries prevention
- More frequent professional cleanings (every 3–4 months for high-risk patients)
- Aggressive dry mouth management
- Application of silver diamine fluoride (SDF) to arrest active root lesions non-invasively
Periodontal Disease and Bone Loss
A lifetime of moderate chronic gum disease — often managed adequately in earlier decades — can reach a tipping point after 60 when reduced immune response, dry mouth, and medications reduce the body’s ability to resist infection. Patients who have maintained stable periodontal health for years may experience acceleration without any change in home care.
Bone levels should be monitored radiographically at every comprehensive examination in older adults. Even patients with no clinical symptoms of active disease can show progressive bone loss on X-rays that warrants a return to more frequent periodontal maintenance.
Oral Cancer: The Risk Rises After 50
The median age of oral cancer diagnosis in the United States is 62. Risk factors include tobacco use (any form), heavy alcohol consumption, and HPV infection. The five-year survival rate is 84% for localized disease and drops to 38% for disease that has spread to lymph nodes — making early detection through systematic oral cancer screening at every dental appointment one of the highest-value clinical activities in geriatric dental care.
Patients over 60 should specifically request a thorough soft tissue examination at every visit and report any oral lesion that does not resolve within two weeks to their dentist promptly.
Dentures and Implants in Older Adults
Many patients in their 60s and 70s present with conventional dentures placed decades earlier that no longer fit properly due to ongoing jawbone resorption. Ill-fitting dentures cause chronic soft tissue irritation, difficulty eating, and nutritional compromise. A denture that fit well at age 55 will typically require relining or replacement by age 70.
Dental implants in healthy older adults have success rates comparable to those in younger patients. Age alone is not a contraindication to implant placement. The relevant factors are bone volume, overall health, and the absence of uncontrolled medical conditions — not the number on a birth certificate. An implant-supported overdenture significantly improves stability, function, and quality of life compared to a conventional denture, and should be discussed with every denture-wearing patient who has not had it evaluated.
Medications and Oral Health Interactions
Calcium channel blockers (amlodipine, nifedipine) — widely prescribed for blood pressure — can cause gingival overgrowth (enlarged gum tissue), which creates plaque traps and complicates home hygiene. Bisphosphonates (used for osteoporosis) are associated with medication-related osteonecrosis of the jaw (MRONJ), a rare but serious complication — patients taking bisphosphonates should inform their dentist before any surgical procedure. Anticoagulants (warfarin, rivaroxaban) require protocol adjustments before extractions or surgical procedures.
Tell your dentist every medication you take at every appointment, including over-the-counter supplements. This information directly affects how we plan and perform your care.
Building a Dental Care Plan for Life After 60
The key principles for oral health management in older adults:
- 3–4 month recall intervals for all patients with gum disease history, dry mouth, or active root caries risk
- Prescription-strength fluoride (5,000 ppm) as the daily toothpaste for high-risk patients
- Comprehensive medication review at every appointment
- Annual oral cancer screening — documented, systematic, thorough
- Proactive discussion of implant options for denture wearers before further bone loss forecloses the option
- Monitoring of aging restorations — proactively replacing failing amalgam before catastrophic fractures occur
Tooth loss is not inevitable with aging. Patients who receive appropriate preventive care, manage dry mouth aggressively, and maintain regular professional supervision keep their natural teeth well into their 80s and 90s. The goal of dental care after 60 is not just treating problems as they arise — it is preventing the cascade of dental disease that occurs when age-related changes go unmanaged.